Why are SVR , SV and SVV of interest?
Function of arteries:
1) Conduits by means of which an adequate supply of blood is delivered
to body tissues
2) Cushions whereby the pulsations resulting from intermittent ventricular
ejection are dampened (thus affects pulse pressure and pulsatile flow)
Mean arterial pressure (MAP) = CO x SVR = ~ peak of curve
CO = height of overall curve in combination with gain
SVR = height of presystolic amplitudes in combination with gain
and in relation to CO
Cushion function: instantaneously accommodation of blood ejected from the
ventricles, storing part of the stroke volume during systole and draining this
volume during diastole, thus permitting continuous perfusion of peripheral
organs and tissues. Influenced by 1) ventricular ejection (SV), 2) arterial
stiffness, 3) wave reflections
Therefore PWA is enabling the practitioner to look for
1) stress related changes: higher PSA due to epinephrine/norepinephrine
effects on arteries (increased SVR), whereas SVV (alternating high and low
single amplitudes) relates to the consequent effects on the myocardium.
2) True hypertension (very high PSA = clearly affected SVR)
3) Stability of sytolic function (SV, SVV)
4) Severity of effects on cardiac output due to mitral regurgitation, dilated
and hypertrophic Cardiomyopathy (SV, SVV)
5) Severity of Arrhythmias (SVV)
6) Activation of RAAS (PSA/SVR), supporting
a. Early diagnosis of kidney disease
b. Early diagnosis of heart disease if no Echo is available
c. Treatment decision on ACE-Inhibitor and other drugs
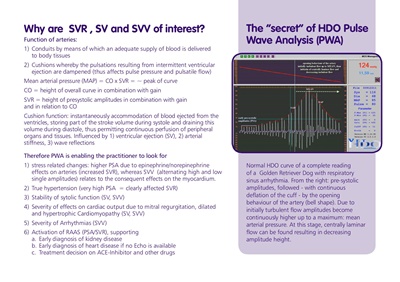
The "secret" of HDO Pulse
Wave Analysis (PWA)
Normal HDO curve of a complete reading
of a Golden Retriever Dog with respiratory
sinus arrhythmia. From the right: pre-systolic
amplitudes, followed - with continuous
deflation of the cuff - by the opening
behaviour of the artery (bell shape). Due to
initially turbulent flow amplitudes become
continuously higher up to a maximum: mean
arterial pressure. At this stage, centrally laminar
flow can be found resulting in decreasing
amplitude height.